Understanding the Crucial Role of Your Osteopathic Doctor in Chronic Pain Management
The problem in front of us-chronic pain—and the practical hope beside it
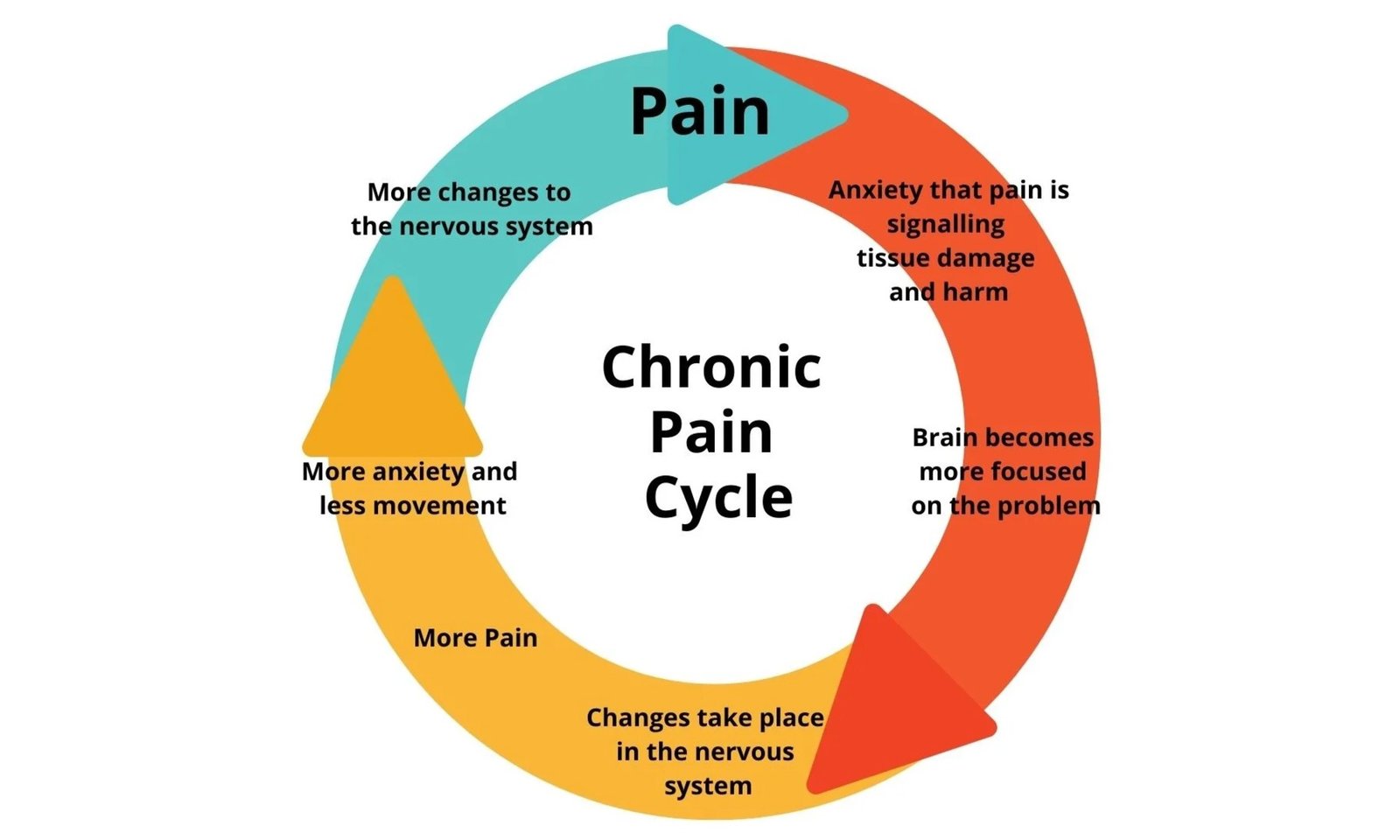
Chronic pain reshapes daily life. It affects sleep, mobility, patience, and participation in family or work routines. Veterans often face added challenges—service-related injuries, deployments, long drives to appointments, and a nervous system conditioned to remain alert.
There isn’t one simple fix. But you can create a plan that respects your duties, schedule, and safety.
Your osteopathic physician (DO) is a fully licensed medical doctor using a whole-person, hands-on approach to improve comfort and function. Many Veterans report easier movement, steadier pacing, and better rest over time, though results vary.
If you and your prescriber explore state-legal medical cannabis, a Medical-Cannabis Care Manager (MCCM) can provide neutral education and handle paperwork logistics. MCCMs are non-clinical—they don’t diagnose, prescribe, or recommend doses, products, or brands.
This roadmap helps you actively participate in your care with clear roles, simple tracking, and realistic steps. You’re not alone—your clinicians, family, and caregivers are part of the support team.
What “osteopathic” can mean for chronic pain
Osteopathic medicine is full-scope medical care (same core training as MDs) with a focus on structure-function relationships. When your ribs, spine, hips, and fascia move more freely, protective muscle bracing decreases, reducing fatigue and improving therapy follow-through.
Your DO may use osteopathic manipulative treatment (OMT)—gentle, low-force techniques aimed at:
- Easing muscle guarding and tension.
- Supporting rib and diaphragm motion for easier breathing and rest.
- Improving circulation and fluid movement to ease stiffness.
OMT is adjusted per visit to fit your condition, energy level, and prescriber’s guidance. It doesn’t replace medications, injections, behavioral therapies, or PT/OT—it complements a coordinated plan.
What a visit may look like
- Review pain triggers, flare-ups, and goals.
- Movement/breathing screen to assess guarding and posture.
- Gentle hands-on care in safe positions to reduce tension.
- Short home routine: positions, micro-breaks, breathing drills.
- Clear “stop rules” for flare days and red-flag symptoms.
What an MCCM does (and doesn’t)
Does:
- Offer neutral education about state-legal programs.
- Help draft questions for your prescriber regarding interactions, duty readiness, or sedation windows.
- Track paperwork, renewals, and deadlines.
- Support consented information flow between clinics.
Doesn’t:
- Diagnose, prescribe, or change medications.
- Provide dosing, product, brand, or potency advice.
- Replace your medical team or suggest skipping labs, imaging, or follow-ups.
Think of an MCCM as an information coordinator. They keep forms organized so clinicians focus on medical decisions while you focus on function and safety.
The 2025 Veteran Roadmap (information-only)
1) Define “better” in concrete terms
Pick 2–3 functional goals you can notice without lab tests:
- Sleep X hours most nights with safer mornings.
- Walk for Y minutes without a crash or long recovery.
- Sit through a class, commute comfortably, or play on the floor with a grandchild.
Write them down. These become shared goals for your team.
2) Build your team—on purpose
- Prescriber (PCP or specialist): diagnosis, medication plan, risk monitoring, and step-downs when appropriate.
- DO: hands-on care, pacing and positioning strategies, breath work, and coordination with PT/OT.
- MCCM (if you pursue cannabis under state law): education/logistics only.
- PT/OT, mental health, peers, family: skills, stamina, and support.
Give everyone the same goals. Ask your clinicians to coordinate when possible.
3) Baseline without blame (1–2 weeks)
Track four numbers (one minute a day):
- Worst pain (0–10)
- Average sleep hours
- Minutes of gentle movement most days
- Number of “bad days” (your definition, used consistently)
Bring these to visits. They tell your story quickly and show trends, even when pain levels vary.
4) Early wins with your DO
Aim for daily comfort and capacity—not heroics:
- Breathing feels easier; shoulders rest lower.
- Guarding eases, making movement smoother with less fear of “catching.”
- Position adjustments at home/work/car reduce strain (chair height, lumbar support, pillow placement).
- Rest routines improve recovery (wind-down patterns, micro-breaks during chores).
As daily comfort improves—and risks stay low—your prescriber may adjust visit frequency or rescue medicines as needed.
5) If you explore medical cannabis (with your prescriber)
- You and your prescriber decide if it’s appropriate, check for interactions, and meet state-specific requirements.
- MCCM handles education and paperwork.
- DO focuses on comfort and mechanics, making tools like PT, mindfulness, and prescribed medicines easier to use consistently.
- No one should pressure you. Laws and workplace rules matter—always ask before you act.
6) Make each day more livable (anti-flare routine)
- Breath that travels: try easy, longer exhales than inhales to reduce tension (with your clinician’s approval).
- Positions that help: small changes in desk, car seat, or sleep setup can take pressure off hot spots.
- Pacing that sticks: a little, often—not a lot, once.
- Sleep that counts: aim for restorative sleep, not just sedation; keep wake-up times steady.
7) Review & adjust (every 2–6 weeks)
Bring your four numbers. If the function trends upward and risks remain low, you and your prescriber may simplify the plan. If things slip, adjust early—don’t wait for a crisis.
Safety boundaries everyone can agree on
- No dosing advice here—prescriber’s responsibility.
- Avoid driving or performing hazardous work after sedating medications or substances.
- Red flags: fever, chest pain, weakness, numbness, shortness of breath, self-harm thoughts, swelling.
- Disclose all meds, supplements, alcohol, and substances.
- Store meds and substances securely.
VA & workplace basics (2025 snapshot—confirm locally)
- VA clinicians can discuss cannabis, but do not prescribe or cover costs. Policies may change; confirm locally.
- Community Care: cannabis certifications and products remain private/out-of-pocket.
- Workplace rules: safety-sensitive roles or federal contractors may test for THC. Plan duty-ready windows with clinicians.
For families & caregivers (you matter)
- Make spaces safe and accessible.
- Celebrate small functional wins.
- Encourage pacing: “a little, often.”
- Guard medications; avoid alcohol/sedative mix.
- Report early changes in mood, mobility, or side effects.
Common Questions
- Will a DO replace my meds? No, DO supports mechanics and pacing; meds remain under the prescriber.
- Do I have to try cannabis? No; optional, state-dependent.
- What about workplace testing? Plan with clinicians to respect rules.
- Can hands-on care flare symptoms? OMT is gentle; alternatives exist.
- How fast will I notice changes? Responses vary; relief can be immediate or gradual.
What to bring to your first DO + (optional) MCCM day
- Top 3 goals in plain language
- Biggest pain triggers and what helps
- Home/work realities affecting pacing/posture
- Full medication/supplement list
- Four baseline numbers
Tracking progress (practical and straightforward)
- One sheet by your bed: days, sleep, worst pain (0–10), movement minutes, “bad day” yes/no.
- Add notes: what helped or hurt, timing of meds or cannabis.
- Review every visit; adjust early if trends slip.
If you and your prescriber explore medical cannabis (brand-neutral, education-only)
- Prefer test-and-review periods over open-ended use.
- Earlier, lower doses reduce grogginess; avoid late, high doses.
- Discuss routes with clinician; non-inhaled forms reduce lung exposure.
- Never mix with alcohol or sedatives unless approved.
- Avoid driving or performing hazardous work within safety windows.
- Pause if nightly use feels necessary; explore non-drug tools.
What progress can look like
- Standing with less bracing
- Calmer, quicker routines
- Walking–resting–walking by design
- Less reliance on “rescue” meds
- Steadier function and fewer spikes
IMPORTANT NOTICE
Educational use only. No medical or legal advice.
Mendry is a 501(c)(3) nonprofit, not a government agency, and not affiliated with the VA or any federal or state agency.
Mendry does not provide treatment, prescribe or sell cannabis, or collect PHI.
Healthcare decisions are yours and your licensed clinicians’ only.
Emergency: 911 | Veterans Crisis Line: 988 (Press 1)